Do you want to get your symbol of feminism back and avoid feeling of incompleteness after removal of breast in breast cancer?
FAQ's
Frequently Asking Question’s on Breast Reconstruction That Comes Up On Patient's Mind
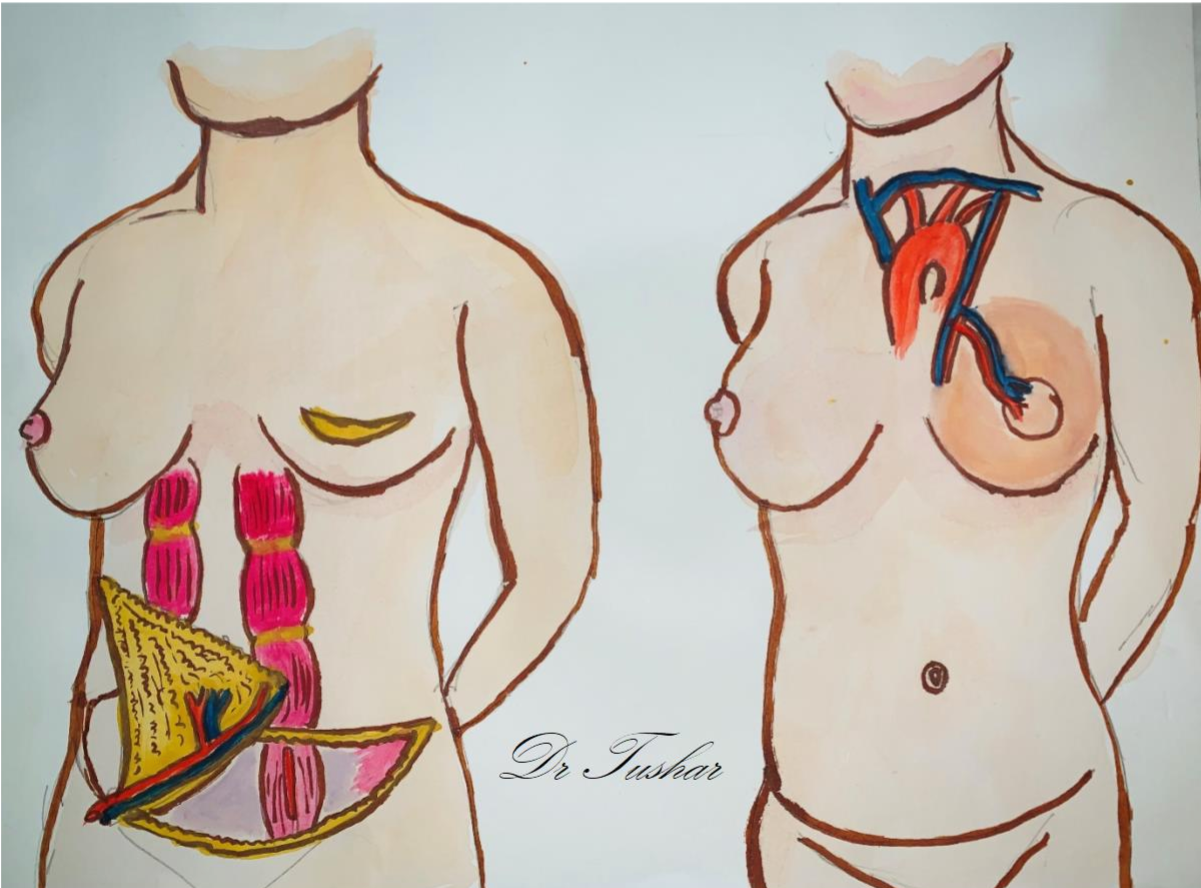
It is complex procedure to restore breast shape and aesthetics after complete breast removal i.e. mastectomy. This procedure involves transfer of tissue from abdomen, back or implant to create new breast mound.
Depending on stage of cancer some part or whole breast is removed in breast cancer. Loss of whole breast or deformed, asymmetrical breast may affect patient psychologically and retain the memories of disease.
Breast reconstruction is performed by plastic surgeon. Patient undergoes thorough evaluation by Plastic surgeon in the form of examination of breasts, deformity assessment, contralateral breast status, Photographic evaluation and expectations. Abdominal laxity, back skin fold thickness and other probable donor sites are examined. Patient is counselled about choice of reconstruction i.e. own body tissue or Implant.
For Aesthetic purpose choice of contralateral symmetrisation procedure is given. Merits and Demerits of no reconstruction with silicon external prosthesis explained.
CT Angiography is required for abdominal tissue is essential for confirmation of blood supply. For implant size and shape opposite breast, skin thickness is taken into consideration.
For Aesthetic purpose choice of contralateral symmetrisation procedure is given. Merits and Demerits of no reconstruction with silicon external prosthesis explained.
CT Angiography is required for abdominal tissue is essential for confirmation of blood supply. For implant size and shape opposite breast, skin thickness is taken into consideration.
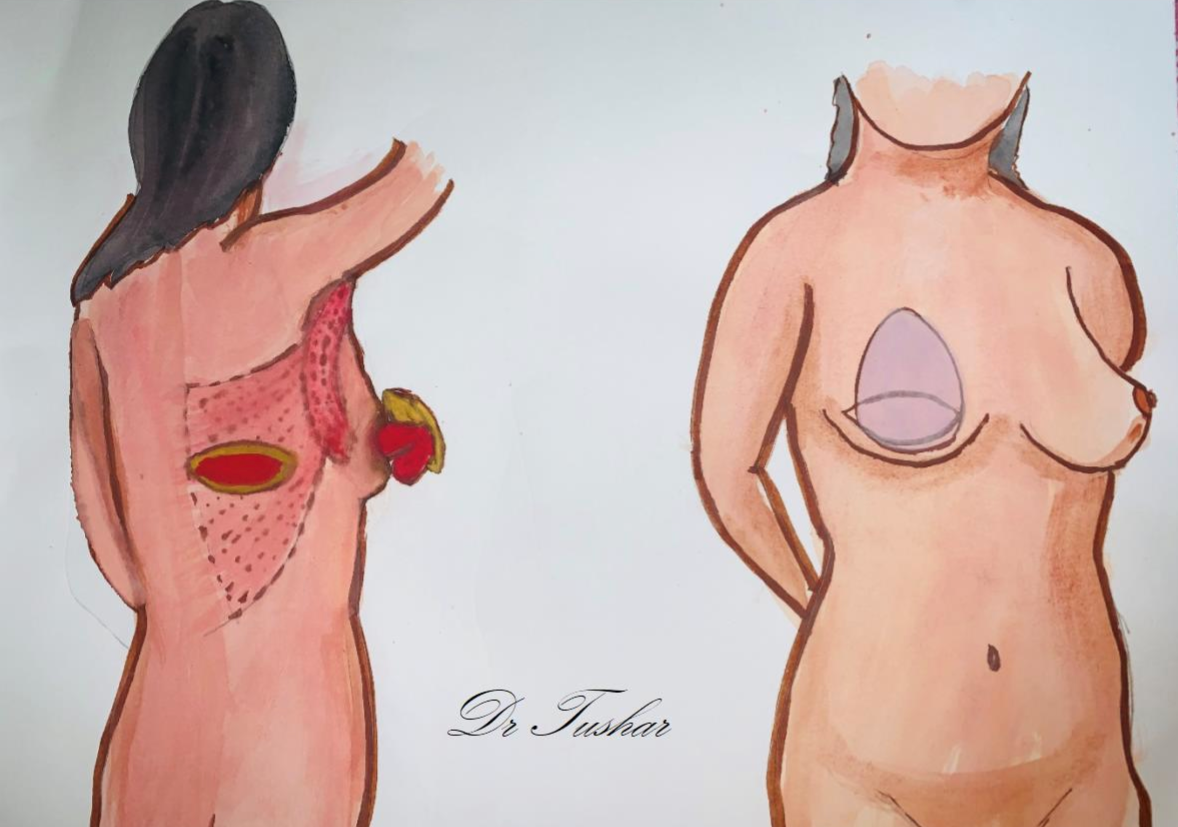
Reconstruction of breast can be done ‘immediately’ during mastectomy or ‘delayed’ as separate procedure later. Advantage of immediate reconstruction is avoidance of second anaesthesia and tissue pliability which may get affected in radiation. Abdominal tissue transfer gives advantage of ‘tummy tuck’ as additional procedure. Most of the time Back tissue is insufficient to provide symmetrical mound necessitates use of silicon implant.
Since it is the choice of patient to get reconstruction done for their comfort, delayed reconstruction is opted after finishing adjuvant chemotherapy or radiotherapy. Delayed reconstruction may involve two stages i.e. first implant expander to negotiate postoperative or radiation related scarring and second stage to complete tissue reconstruction or Implant.
Since it is the choice of patient to get reconstruction done for their comfort, delayed reconstruction is opted after finishing adjuvant chemotherapy or radiotherapy. Delayed reconstruction may involve two stages i.e. first implant expander to negotiate postoperative or radiation related scarring and second stage to complete tissue reconstruction or Implant.
Reconstruction with abdominal tissue takes 8 to 10 hrs of surgical procedure. 5-7 days of hospital stay for flap monitoring and dressing is needed. Back tissue reconstruction with or without Implant takes 4-5 hrs of operative time. Patient can be discharged on 3-5 days postop. Drain tubes are kept under the skin to evacuate collected fluid which can be removed with decreased daily count (<30 ml)
Breast reconstruction is process of forming new breast mound. There are no sensations or functions in reconstructed breast. Although new breast won't look exactly like natural one did, the contour of
breast can usually be restored. Thus it helps patient psychologically and tries to erase the memories of cancer
· Infection
· Bleeding
· Prolonged time in surgery and under anesthesia
· Extended recovery and healing time
· Fluid collection (seroma)
· Tissue death (necrosis) due to insufficient blood supply
· Fat necrosis
· Abdominal wall hernia or weakness
· Bleeding
· Prolonged time in surgery and under anesthesia
· Extended recovery and healing time
· Fluid collection (seroma)
· Tissue death (necrosis) due to insufficient blood supply
· Fat necrosis
· Abdominal wall hernia or weakness
· Infection
· Bleeding
· Seroma
· Implant exposure
· Capsular Contracture
· Asymmetry of breast
· Bleeding
· Seroma
· Implant exposure
· Capsular Contracture
· Asymmetry of breast
No, recent advances in MRI and Mammography are useful in detecting early changes in reconstructed breast
Patient can join the regular activities in two weeks of surgery. Reconstruction with abdominal tissue restrains vigorous exercises, weight lifting for 3 months. Use of back tissue with or without implant per say does not restrict any exercise, But it may affect person doing mountain climbing.
Patient needs to come for follow up for suture removal after 10 days of surgery. Thereafter patient comes after 1 month, 3 month and 6 monthly for follow up. Patient is advised to wear sports bra which can help in reducing swelling and support the breast while it heals. When abdominal tissue is used patient has to bend forward while walking for 7 days and use abdominal binder while walking for 1 month.
Radiation delivered to chest may affect local vascularity. Thus nipple reconstruction is done after 6-8 months of surgery. Areola Tattooing follows to this for aesthetic reconstruction.
If Expander implant is used for reconstruction, it is deflated during radiation. Permanent silicon implant is inserted after appropriate expansion of about 3 months of radiation.
If Expander implant is used for reconstruction, it is deflated during radiation. Permanent silicon implant is inserted after appropriate expansion of about 3 months of radiation.
Aesthetic reconstruction warrants symmetrical breasts. Patient with droopy opposite breast gets benefit of breast lift during same anaesthesia and it looks better. Patient with smaller opposite breast gets benefit of implant or fat injection for symmetrical breast reconstruction.